Alcohol in
Moderation
Moderation
Larsson, S.C., Mason, A.M., Cronjé, H.T., Bassett, E., Horta, G., Kar, S., Burgess, S. BMC Medicine (2025) 23:676
doi.org/10.1186/s12916-025-04543-8
Abstract
Background: Alcohol consumption has been linked to cancer risk. Evidence is strongest for seven cancer types: breast, colorectum, oesophagus, liver, mouth, pharynx, and larynx. However, evidence supporting a causal effect from Mendelian randomization is inconsistent.
Methods: We perform a comprehensive Mendelian randomization analysis to assess whether genetically predicted alcohol consumption associates with risk of 20 cancers. Such associations would provide supportive evidence for a causal effect of alcohol consumption on cancer risk. We used 95 genetic variants associated with alcohol consumption at genome-wide significance. Primary analyses were conducted in European ancestry participants from UK Biobank (367,643 individuals), FinnGen (500,348 individuals), All of US (169,312 individuals), and Million Veteran Program (451,206 individuals). We also estimated associations in cancer-specific consortia.
Results: No association was observed between genetically predicted alcohol consumption and overall cancer (odds ratio (OR) per 1 standard deviation increase in alcohol consumption 0.96, p = 0.45). Among the seven highlighted cancer types, we saw a multiply-corrected significant positive estimate for combined head/neck cancer (OR 1.51, p = 0.001), and nominally significant positive estimates for colorectal (OR 1.21, p = 0.035) and oesophageal (OR 1.42 p = 0.033) cancer. For liver cancer, there was a null estimate overall (OR 1.40, p = 0.10), but a nominally significant positive estimate in Million Veteran Program and when using the ADH1B-rs1229984 variant. For breast cancer, there was a null estimate in biobank data (OR 1.09, p = 0.25) and consortium data (OR 0.98, p = 0.84). Conversely, we observed multiply-corrected significant negative estimates for kidney cancer (OR 0.64, p = 0.0003) and endometrial cancer (OR 0.56, p = 0.0006), and nominally significant negative estimates for non-Hodgkin’s lymphoma (OR 0.75, p = 0.010), myeloma (OR 0.61, p = 0.014), and some subtypes of ovarian cancer. There was a nominally significant positive association with cancer mortality (OR 1.44, p = 0.003), although this attenuated on adjustment for smoking heaviness. Limitations include potential invalidity of the genetic variants as instruments, limited power, multiple testing, variable cancer detection rates, and unrepresentativeness of the datasets.
Conclusions: We observed moderate-to-weak evidence supporting causal effects of alcohol consumption on risk of head/neck, oesophageal, and colorectal cancer, inconsistent evidence for liver cancer, and no evidence for breast cancer. Overall, human genetic data do not provide evidence that alcohol consumption is a cause of all cancers and suggest there may even be inverse associations with certain cancer types.
ISFAR Summary
The relationship between alcohol consumption and cancer remains a pivotal topic. Larsson et al. (2025) present an impressive paper that attempts to associate alcohol consumption with cancer risk, defining alcohol consumption using genetic information.
Overall, several cancer types were positively associated with alcohol consumption, and several were negatively associated. Most of the positive and negative associations were consistent with classical state-of-the-art epidemiology. Surprisingly, there appeared to be no overall positive association between alcohol consumption and the incidence of any cancer type, and no association between alcohol consumption and breast cancer risk, neither overall nor for any of the subtypes studied.
In their discussion section, the authors adopt a highly critical stance towards their findings and the MR methodology used. They list numerous limitations in their analyses, one of which is that the genetic variants used to define alcohol consumption explain only approximately 0.2% of the variability in alcohol consumption, a figure that is extremely low. This may mean that cause-and-effect relations between alcohol consumption and overall cancer risk cannot be assessed by MR techniques, as the authors conclude: “Overall, human genetic data do not provide evidence that alcohol consumption is a cause of all cancers and suggest there may even be inverse associations with certain cancer types.”
Unfortunately, very large and extensive MR studies of the relation between alcohol and cancer continue to be published, while genetic information defining alcohol consumption generally accounts for a minimal part of that alcohol consumption.
Background
The relationship between alcohol consumption and cancer remains a pivotal topic. This became important in the late 1980s, when the International Agency for Research on Cancer (IARC), a WHO institute, classified alcoholic beverages as Group 1 carcinogens, indicating sufficient evidence of their carcinogenicity in humans. In addition, IARC considers there to be sufficient evidence of carcinogenicity in experimental animals, combined with strong mechanistic evidence of carcinogenicity in humans. Evidence is strongest for several cancers, including those of the mouth, throat, liver, breast, and bowel. Subsequently, several other organisations have followed IARC’s classification, stating that any alcohol consumption can cause cancer. , .
The issue remains debated, as the alcohol-cancer relationship in humans is based mainly on epidemiological associations. Although numerous interventions have been conducted in animals, no long-term intervention studies in humans have been performed to show that alcohol consumption is carcinogenic. It is even unlikely that a large-scale randomised trial would be feasible or ethical to conduct.
Another important issue in the discussion is the dose of alcohol consumed. The IARC and the WHO consider any alcohol consumption to increase the risk of cancer. However, several of the cancers for which the association with alcohol consumption is strongest, such as mouth, throat, liver and bowel, occur only at high to very high consumption levels. Apart from the average dose of alcohol consumed, other alcohol consumption behaviours and lifestyle factors are considered essential for cancer risk. Specifically, for those cancers for which the risk increase is relatively small at low doses, such as breast cancer, other lifestyle factors may have confounded the observed associations.
Low-dose alcohol consumption, often referred to as light to moderate alcohol consumption, is difficult to assess accurately in epidemiological studies on which the alcohol-cancer association has been based. Alcohol consumption is usually assessed by questionnaire, which may lead to underestimation. In addition, alcohol consumption may have been evaluated on a limited number of occasions over a long follow-up. Furthermore, those who have been drinking heavily in the past but do not drink anymore may confound associations further.
Larsson et al. (2025) is interesting in this respect. The impressive paper attempts to associate alcohol consumption with cancer risk and defines alcohol consumption based on genetic information. Genetically predicted alcohol consumption, estimated using Mendelian Randomisation (MR) analysis, would provide supportive evidence for a causal relationship between alcohol consumption and cancer risk. Although genetic make-up may theoretically predispose to alcohol consumption, it is hard to imagine that such a specific behaviour will be completely determined by genetic make-up, with social conditions and cultural factors contributing nothing at all. This makes MR yet another tool that incompletely assesses whether alcohol consumption is associated with health outcomes.
Critique
The study used data from four large longitudinal epidemiological studies, comprising more than 1.5 million participants in Europe and the USA, to assess cancer risk. Additional datasets were used to analyse specific outcomes, including breast cancer, overall, and 20 cancer types defined by cancer site, as well as some composite outcomes. The authors performed various MR analyses using genetic variants previously shown to be associated with alcohol consumption in a large genome-wide association study. Several adjustments were made to the variants used due to missing data, duplicates, and high correlation among variants.
As with many large biobank-based analyses, potential selection bias should be acknowledged. Participants in cohorts such as the UK Biobank tend to be healthier and consume less alcohol than the general population, which may attenuate both observational and genetically predicted associations, particularly at higher levels of alcohol consumption.
Overall, several cancer types were positively associated with alcohol consumption, and several were negatively associated. Most of the positive associations were consistent with classical state-of-the-art epidemiology, namely colorectal cancer, head/neck cancer and oesophageal cancer. Also, most of the negative associations were consistent with classical state-of-the-art epidemiology, namely, kidney cancer (Song et al., 2012), myeloma cancer (Rota et al., 2014) and non-Hodgkin lymphoma (Tramacere et al., 2012). However, consistency between MR findings and observational reports of inverse associations should be interpreted cautiously. Inverse MR estimates are particularly vulnerable to horizontal pleiotropy, selection bias, and correlated metabolic or lifestyle pathways, and should not be interpreted as evidence of a protective effect of alcohol consumption.
An odd one out is the positive association between alcohol consumption and lung cancer, which was reported to be either not associated or negatively associated, depending on the adjustment for smoking (Fehringer et al., 2017, Rohrmann et al., 2006). Larsson et al. (2025) also found a sharp attenuation of the association.
Surprisingly, there appeared to be no overall positive association between alcohol consumption and the incidence of any cancer type. This is interesting, since health organisations promote the idea that any alcohol consumption will increase the risk of cancer. This message may stem from positive associations with some cancers, but when all major cancers are considered, the overall risk is not significant. Some authors have reached a similar conclusion when both the positive and negative associations for various cancer types are taken into account (Hendriks & Calame, 2018).
A similar conclusion, no association, was reached regarding the association between alcohol consumption and breast cancer risk, neither overall nor for any of the subtypes studied. This finding is inconsistent with meta-analyses of observational studies, which show a 5% to 10% increase in breast cancer risk per 10 g alcohol per day increment (Hamajima et al., 2002), but is consistent with several other meta-analyses (Kumar et al., 2024, Lim et al., 2025). The authors do not discuss this discrepancy in detail, beyond suggesting the possibility of residual confounding in observational studies or that their analyses have insufficient statistical power to detect such modest associations.
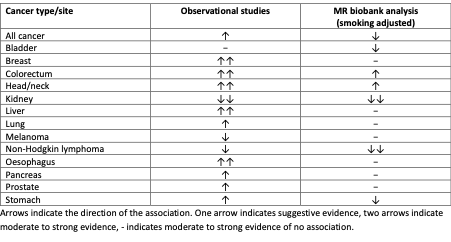
Table: Comparison of results from observational studies and the current MR study based on Table 3 in Larsson et al. (2025).
In their discussion section, the authors adopt a highly critical stance towards their findings and the MR methodology used. Firstly, they state: “We want to leave readers in no doubt that alcohol consumption increases the risk of many diseases.” While this statement is broadly accurate, additional nuance regarding alcohol consumption levels and drinking patterns would have been helpful. Secondly, the authors note that readers of their paper are often less sceptical of their findings than the authors themselves are, and they then list numerous limitations in their analyses. This limitation is also reflected in their observation that the genetic variants used explain only approximately 0.2% of the variability in alcohol consumption, a figure that is extremely low.
We agree that MR analyses may be less informative than classical state-of-the-art epidemiology for complex behavioural exposures such as alcohol consumption, primarily because a person’s genetic make-up captures only a limited proportion of individual drinking behaviour, including patterns, timing, and consumption context. In addition, MR analyses typically assume linear exposure–outcome relationships. If alcohol-related cancer risk is non-linear, threshold-dependent, or driven by specific patterns such as heavy episodic drinking or exposure during hormonally sensitive life stages, such effects may not be adequately captured by current genetic instruments.
This may mean that cause-and-effect relations between alcohol consumption and overall cancer risk cannot be assessed by MR techniques, as the authors conclude: “Overall, human genetic data do not provide evidence that alcohol consumption is a cause of all cancers and suggest there may even be inverse associations with certain cancer types.”
ISFAR has recently evaluated two other papers assessing the relationship between alcohol consumption and cancer risk, namely (Zhu et al., 2020) and (Sohi et al., 2024).
Compared with Larsson et al. (2025), who examined 20 cancers across broader sites, Zhu et al. (2020) focused on hormone-dependent cancers, specifically breast and ovarian cancers. They used a two-sample MR with three alcohol exposure measures — drinks per week, alcohol use disorder (AUD), and AUDIT-C (an adjusted measure of drinking behaviour). They found no evidence of a causal effect of genetically predicted alcohol consumption on breast cancer risk consistent across any of the three exposure measures. For the breast cancer subtypes ER+ and ER–, they also found null results across exposures. For ovarian cancer, they found a borderline reduced risk with one instrument (AUDIT-C), but this disappeared when excluding variants associated with possible confounders. Overall, there was no robust evidence of a causal effect.
By contrast, the study by Sohi et al. (2024) was a systematic review and meta-analysis of prospective observational studies, rather than an MR study. The authors reported that alcohol consumption increases the risk of female breast cancer, even at low levels of approximately one drink/day, and that a dose–response relationship was observed across drinking categories.
These differences in studies are important. Observational studies adjust for known confounders but remain vulnerable to residual confounding and measurement error. MR studies aim to strengthen causal inference by using genetic proxies to mitigate confounding, but they are insensitive to drinking patterns and rely on key assumptions, including the absence of horizontal pleiotropy.
MR evidence from both Larsson et al. (2025) and Zhu et al. (2020) does not support a strong causal link between alcohol consumption and breast cancer. This suggests that the observational association reported by Sohi et al. (2024) may be influenced by residual confounding (e.g., smoking, diet or hormone therapy use) or that MR instruments fail to capture relevant aspects of alcohol exposure, such as timing, patterns and heavy episodic drinking. The discrepancy, therefore, likely reflects differences in methodology and in what each approach can detect, underscoring the importance of integrating genetic, mechanistic and observational evidence when interpreting alcohol–cancer relationships.
Specific comments
Forum member Ellison comments that “MR may have a role in relating alcohol to some cancers but probably provides less information for the association with cancers that are strongly related to lifestyle factors, especially drinking habits and smoking. It appears that the estimate of actual alcohol intake tends to be better from self-reports than from genetic factors associated with intake. This suggests that for cancers less related to drinking habits or other lifestyle factors, the finding of significant associations of alcohol with, for example, kidney cancer and haematological cancers, might be more informative.”
There continue to be a plethora of very large and extensive MR studies of the relation between alcohol and cancer, even though (as stated by the authors) the instrumental factors used in MR generally play only a minimal role in judging alcohol consumption, explaining only a tiny proportion of its variability. Yet numerous studies of the health effects of alcohol consumption continue to be reported. For some reason, it seems to me that there are now fewer studies relating smoking to cancer, even though the effects on risk are much larger than they are for alcohol consumption. Further, there continue to be frequent studies of alcohol, but none, if any, on the effects, for instance, of milk or of lemonade on the risk of cancer. This may, to some extent, be because there are few ‘anti-milk’ or ‘anti-lemonade’ investigators out there!
I agree with the authors’ extensive discussion of the limitations of this study’s results. This paper provides data for each of a large number of cancers, not just for all cancers combined. This is the correct approach, as there are presumably many factors involved in the risk of cancer, and they may vary markedly for each type of cancer. This means that a lack of relation between alcohol and total cancer risk does not necessarily rule out strong effects on specific types of cancer. However, the extensive scientific literature to date continues to suggest that, except for upper gastrointestinal and liver cancers, which are seen more frequently among alcohol abusers, moderate drinking plays a minor role in the aetiology of most cancers and even reduces the risk for some.
Forum member Harding considers “the overall findings of the Larsson et al. (2025) study are, with some exceptions, broadly consistent with those of observational epidemiology in the relationship between alcohol consumption and various cancers. The Review of Evidence on Alcohol and Health, conducted by the US National Academies of Sciences (2025) to inform the 2025-2030 Dietary Guidelines for Americans (2026), is a further recent contribution to the debate. In short, it is hard to discern an overall clear consensus on the relationship between alcohol consumption and various cancers, in contrast to the relationship between moderate alcohol consumption and the spectrum of cardiovascular diseases and diabetes, for example.
In describing the background to the study, the researchers put it in the context of the 2025 US Surgeon General’s Advisory on Alcohol and Cancer (2025), which very clearly identified alcohol as the third leading preventable cause of cancer in the US, after tobacco and obesity. They can’t both be right.
The rationale in the US Surgeon General’s Advisory appears to be
there are a number of biologically plausible mechanisms by which alcohol could cause cancer in humans, and
therefore, alcohol causes cancer in those who consume it.
Further, the US Surgeon General’s Advisory is particularly cavalier in regarding statistical associations found in epidemiological studies between alcohol consumption and particular cancers as causal. On page 7, the US Surgeon General’s Advisory acknowledges the importance of determining whether an observed association is causal by application of ‘well-established scientific criteria such as the Bradford-Hill criteria’, but does not cite even one example where these criteria have actually been applied. For this reason alone, in my view, the US Surgeon General’s Advisory should be regarded as unconvincing, at best. The studies that show an apparent protective effect of alcohol consumption on the incidence of some cancers are simply ignored.
Larsson et al. (2025) suggest a much more nuanced relationship between alcohol consumption and cancer. This is much more likely to be closer to the truth.”
Forum member Skovenborg “still does not quite understand how an analysis of the effect of alcohol that explains only approximately 0.2% of the variability in alcohol consumption may yield sound and informative results. I am also sceptical about organisations that quote the results of MR studies showing no evidence for a beneficial effect of alcohol consumption on cardiovascular disease, without mentioning the result of no association between genetically predicted alcohol consumption and breast cancer overall, for any subtype of breast cancer, or for breast cancer survival.
A great problem is the lack of information about drinking patterns such as drinking with meals vs fasting and regular, light drinking vs. binge-type drinking. MR studies have no information at all, and only a few observational studies have asked questions about drinking patterns. Effect modification by drinking pattern has been reported in several studies. For example, Ma et al. (2021) defined a healthy drinking habit score (DHS) as regular drinking (frequency of alcohol intake ≥ 3 times/wk) and consuming alcohol with meals (participants who indicated they drink alcohol with meals). After adjustment for potential confounders and the amount of alcohol consumed, regular drinking (frequency of alcohol intake ≥ 3 times/week) was significantly associated with a 7% lower risk of all-cause mortality (HR, 0.93; 95% CI, 0.88-0.99) and an 8% lower risk of cancer mortality (HR, 0.92; 95% CI, 0.85-0.99) compared with nonregular drinking (frequency of alcohol intake <3 times/week). Similarly, compared with participants who consumed alcohol outside meals and those with varying patterns, participants who consumed alcohol with meals had a significantly 12% lower risk of all-cause mortality (HR, 0.88; 95% CI 0.84-0.93), a 13% lower risk of CVD mortality (HR, 0.87; 95% CI, 0.78-0.97), a 10% lower risk of cancer mortality (HR, 0.90; 95% CI 0.85-0.95), and a 14% lower risk of other-cause mortality (HR, 0.86; 95% CI 0.78-0.94). For cancer mortality, a positive linear association was observed in participants with unfavourable DHS, whereas a J-shaped association was observed in participants with favourable DHS. Of note, moderate alcohol intake (50-200 g/week) was not associated with cancer mortality in participants with favourable DHS.”
References
References
Fehringer, G., Brenner, D. R., Zhang, Z. F., Lee, Y. A., Matsuo, K., Ito, H., Lan, Q., Vineis, P., Johansson, M., Overvad, K., Riboli, E., Trichopoulou, A., Sacerdote, C., Stucker, I., Boffetta, P., Brennan, P., Christiani, D. C., Hong, Y. C., Landi, M. T., … & Hung, R. J. (2017). Alcohol and lung cancer risk among never smokers: A pooled analysis from the International Lung Cancer Consortium and the SYNERGY study. International Journal of Cancer, 1, 140(9), 1976-1984 doi.org/ 10.1002/ijc.30618.
Hamajima, N., Hirose, K., Tajima, K., Rohan, T., Calle, E. E., Heath Jr., C. W., Coates, R. J., Liff, J. M., Talamini, R., Chantarakul, N., Koetsawang, S., Rachawat, D., Morabia, A., Schuman, L., Stewart, W., Szklo, M., Bain, C., Schofield, F., Siskind, V., … & Collaborative Group on Hormonal Factors in Breast, C. (2002). Alcohol, tobacco and breast cancer–collaborative reanalysis of individual data from 53 epidemiological studies, including 58,515 women with breast cancer and 95,067 women without the disease. Br J Cancer, 87(11), 1234–1245. doi.org/10.1038/sj.bjc.6600596
Hendriks, H. F. J., & Calame, W. (2018). The contribution of alcohol consumption to overall cancer incidence in the Western World: a meta-analysis. Journal of Nutrition and Health Sciences, 5(3), 311.
Kumar, N., Ehsan, S., Banerjee, S., Perez, C. F., Lhuilier, I., Neuner, J., Friebel-Klingner, T., Fayanju, O. M., Nair, B., Niinuma, S. A., Nampoothiri, S., & McCarthy, A. M. (2024). The unique risk factor profile of triple-negative breast cancer: a comprehensive meta-analysis. Journal of the National Cancer Institute, 116(8), 1210–1219. doi.org/10.1093/jnci/djae056
Lim, G. H., Tan, Y. C. R. S., Lee, E., Loo, C. K. Y., Kumar, N., Chong, M. F. F., & Chia, A. (2025). Adolescent Dietary Intake and Breast Cancer in Adulthood: A Systematic Review and Meta-analysis. Advances in Nutrition, 16(10). doi.org/10.1016/j.advnut.2025.100503
Ma, H., Li, X., Zhou, T., Sun, D., Shai, I., Heianza, Y., Rimm, E.B., Manson, J.E., & Qi, L. (2021) Alcohol consumption levels as compared with drinking habits in predicting all-cause mortality and cause-specific mortality in current drinkers. Mayo Clinic Proceedings, 96(7), 1758-1769. doi.org/10.1016/j.mayocp.2021.02.011.
National Academies of Sciences, Engineering, and Medicine (2025) Review of evidence on alcohol and health. Washington, DC: The National Academies Press. doi.org/10.17226/28582.
Office of the Surgeon General (US). Alcohol and Cancer Risk: The U.S. Surgeon General’s Advisory [Internet]. Washington (DC): US Department of Health and Human Services; 2025. PMID: 40367254.
Rohrmann, S., Linseisen, J., Boshuizen, H. C., Whittaker, J., Agudo, A., Vineis, P., Boffetta, P., Jensen, M. K., Olsen, A., Overvad, K., Tjonneland, A., Boutron-Ruault, M. C., Clavel-Chapelon, F., Bergmann, M. M., Boeing, H., Allen, N., Key, T., Bingham, S., Khaw, K. T., … Riboli, E. (2006). Ethanol intake and risk of lung cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). American Journal of Epidemiology, 164(11), 1103–1114. doi.org/10.1093/aje/kwj326.
Rota, M., Porta, L., Pelucchi, C., Negri, E., Bagnardi, V., Bellocco, R., Corrao, G., Boffetta, P., & La Vecchia, C. (2014). Alcohol drinking and multiple myeloma risk–a systematic review and meta-analysis of the dose-risk relationship. European Journal of Cancer Prevention: The Official Journal of the European Cancer Prevention Organisation (ECP), 23(2), 113–121. doi.org/10.1097/CEJ.0000000000000001
Sohi, I., Rehm, J., Saab, M., Virmani, L., Franklin, A., Sánchez, G., Jhumi, M., Irshad, A., Shah, H., Correia, D., Ferrari, P., Ferreira-Borges, C., Lauby-Secretan, B., Galea, G., Gapstur, S., Neufeld, M., Rumgay, H., Soerjomataram, I., & Shield, K. (2024). Alcoholic beverage consumption and female breast cancer risk: A systematic review and meta-analysis of prospective cohort studies. Alcohol, Clinical & Experimental Research, 48(12), 2222–2241. doi.org/10.1111/ACER.15493
Song, D. Y., Song, S., Song, Y., & Lee, J. E. (2012). Alcohol intake and renal cell cancer risk: a meta-analysis. British Journal of Cancer, 106(11), 1881–1890. doi.org/10.1038/bjc.2012.136
Tramacere, I., Pelucchi, C., Bonifazi, M., Bagnardi, V., Rota, M., Bellocco, R., Scotti, L., Islami, F., Corrao, G., Boffetta, P., La Vecchia, C., & Negri, E. (2012). Alcohol drinking and non-Hodgkin lymphoma risk: a systematic review and a meta-analysis. Annals of Oncology, 23(11), 2791–2798. doi.org/10.1093/annonc/mds013
US Department of Agriculture. Dietary Guidelines for Americans, 2025-2030. Accessed January 9, 2026. cdn.realfood.gov/DGA.pdf
Zhu, J., Jiang, X., & Niu, Z. (2020). Alcohol consumption and risk of breast and ovarian cancer: A Mendelian randomization study. Cancer Genetics, 245, 35–41. doi.org/10.1016/j.cancergen.2020.06.001.
Comments on this critique by the International Scientific Forum on Alcohol Research were provided by the following members:
Henk Hendriks, PhD, Independent consultant and partner of the Nutrition Consultants Cooperative, Netherlands
Creina Stockley, PhD, MBA, Independent consultant and Adjunct Senior Lecturer in the School of Agriculture, Food and Wine at the University of Adelaide, Australia
R. Curtis Ellison, MD, Section of Preventive Medicine/Epidemiology, Boston University School of Medicine, Boston, MA, USA
Richard Harding, PhD, Formerly Head of Consumer Choice, Food Standards and Special Projects Division, Food Standards Agency, UK
Erik Skovenborg, MD, specialized in family medicine, member of the Scandinavian Medical Alcohol Board, Aarhus, Denmark